
LMHI 2015 RIO DE JANEIRO
Abstract
The similia law is the fundamental pillar of homeopathy and Hahnemann tried to explain it with the pharmacological examples of Organon par. 65, regarding coffee, opium and wine. Fortier-Bernoville in the 1930s introduced the notion of ‘reverse action’ of low doses in respect to high doses, following the rule of stimulant action of low doses of poisons stated by Arndt and Schulz in 1888. This rule biased the discussion on Similia law with the previously unknown idea of an inversion of effect with dilutions, which became a comprehensible model to represent the similitude. Nothwithstanding hormesis and homeopathy share some analogies, important distinctions are present, first of all the concept of different responses between health and disease states, absent in hormesis and basic in homeopathy.
Years later, the discovery of receptors’ importance in drug activity put another obstacle to biologically understand Similia law. This was mainly caused by two significant, but subsequently updated, misinterpretations about receptors: 1) the beliefs that receptors have fixed number and sensitivity to drugs were changed in a great receptor plasticity after drug binding for homeostatic reactions which change cell responses, 2) the idea they react only to chemical signals was corrected by evidences of their activation by light, temperature and e.m. fields. If the latter point may now open the possibility of action of infinitesimal doses at receptor level, the discovery of membrane receptor homeostatic plasticity justifies the occurrence of temporal opposite symptoms after a drug intake due to internalization from or re-insertion to membrane of receptor molecules which change dramatically cell responses and symptoms. All physical, behavioral or emotional symptoms are indeed directly or indirectly caused by constitutive or ligand-dependent receptor activity, through their activation, inhibition or modulation. A new vision which includes opposite symptoms and receptor-dependent rebound effects after drug administration, may disclose the hypothesis of a therapeutic rebound effect (TRE) using similar drugs, independently of the dosage used. Doseindependence must be present considering that similia law was born with ponderal doses. Adjunctively such vision may explain two important homeopathic phenomena of clinical follow-up: the initial aggravation of symptoms and the return of old symptoms.
An important verification of this hypothesis must include the biological description of the three examples Hahnemann provided to explain similia therapy. Here we show the pharmacological analysis of the opposite symptoms described for coffee, opium and wine. We found that all secondary symptoms of these drugs are due to receptor homeostatic plasticity in opposite direction to drug effects for a vital defence organized by living beings. This opposite reaction to drugs is a general phenomenon in most receptors and for most common drugs, both agonists or inverse agonists, which may account for the term law, a law, until now, not recognized.
Introduction:
Homeopathy has reached a great diffusion in the world, notwithstanding there is a poor consensus on its biological foundation, both because similitude is counterintuitive and effects of ultra-dilutions appear implausible. Adjunctive difficulties lay in understanding Hahnemann’s homeopathic basic principles, the primary and secondary actions of drugs: after a strong dose of drug secondary symptoms are a) successive in time to primary symptoms, b) opposite to the main drug action and c) due to a body reaction and not primarily to drug effect [1]. Just one year after Hahnemann’s death Hering criticized the statement of the primary and secondary actions of the drugs and rejected some conclusions [2]. The discussion continued uncertainly between homeopaths until Fortier-Bernoville [3] in the 1930s gave a new comprehensible interpretation on similitude: high dilutions of drugs invert the direction of drug effects, deducible by the fact that sometimes low doses have opposite effects in respect to high doses. The nature of this inversion is still enigmatic and not consistent with opposite actions to primary drug effects observed in function of the time, after a single high dose, without changing quantity of the drug [1]. A further obstacle to accept that homeopathy might be based on a natural law [4] occurred when receptor proteins were discovered. Receptors were initially believed to be invariant, passive, totally dependent on a drug binding and metaphorically represented with the ‘key-lock model’. Drug effects were found to be dose-dependent, decreasing with the decrease of the drug dose and increasing with its increase. In this way the organism reaction was totally absent and the possibility for a biological action of the infinitesimal doses precluded. The image of these receptor features is as persisting in most physicians’ belief as it is obsolete. If we suppose that homeopathy has local physicochemical effects and it is not a metaphysical phenomenon [4] we have to include receptors in a discussion on symptoms, because symptoms, physical, behavioral or emotional, are the final result of drug effects which are mediated by receptor activities [5]. Only when we could not find any rationale, so we have to think to non-local effects [6]. Fortunately the two most important biological impediments to develop a biological hypothesis for homeopathy, that is the absence of homeostatic reactions to drugs (see after) and the insensitivity of cells to physical inputs have been shown untruth [7-9]. I try to show here how the novel perspectives on receptor functioning allow to rescue the first homeopathic principle from a biological point of view: homeopathy could be interpreted as a rebound therapy, due to some biological reactive property of the cells to chemical compounds.
Homeopathy, biology and receptors: Pharmacological evidences now account for a new receptor model with unexpected characteristics. For instance they are not passive and produce effects in absence of agonist, they have a constitutional activity, a basal activity in absence of any ligand [10]. Moreover most antagonists produce effects even without the presence of agonist, while it was previously thought that antagonists may only counteract agonist binding. Antagonists are now termed inverse agonists. Receptors are very dynamic structures and may change their surface density inversely to pharmacological stimuli (Fig.1), decreasing it when bound to a stimulant drug (agonist) – receptor endocytosis in cytoplasmatic vesicles- (Fig 1B) or increasing it when bound to an inhibiting drug (antagonist or inverse agonist) – receptor incorporation to the membrane surface [11-12] (Fig 1C). These dynamics of receptor trafficking potently control the sensitivity to drugs and onset of symptoms. Manipulation of receptor number or activity occur rapidly and very frequently, but not constantly, during a drug therapy in the opposite sense of the drug action, for homeostatic defence and lead to tolerance. The same mechanisms of receptor adaptations lead to withdrawal syndromes, as in beta blocker withdrawal which induces a crescendo angina due to beta-receptor up-regulation [13] (Fig 1C) or after benzodiazepines use (BDZ). In anxious patients GABAA receptors are probably down-regulated [14]. Their activation by BDZs initially calms anxiety, but it may produce additional agonist-induced down-regulation (Fig. 1B) [15]. This explains because, after BDZ discontinuation, symptoms are more perceptible than before if the subject stops the intake.
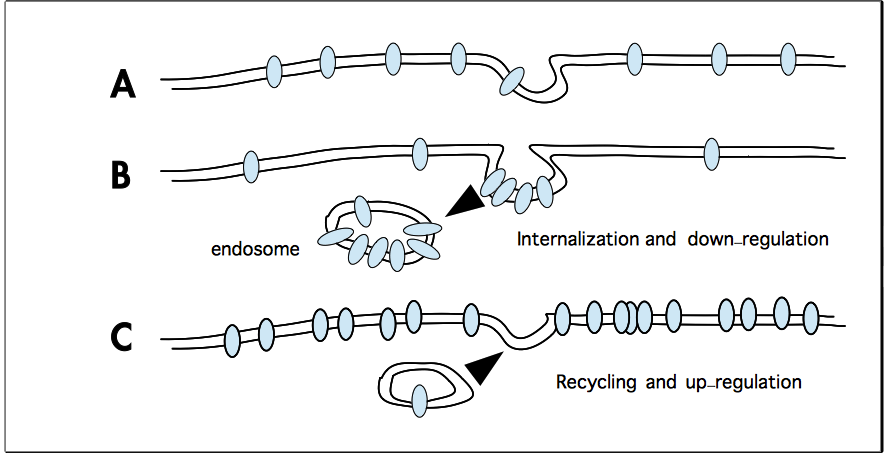
Fig. 1: the figure illustrates the change of receptor expression and density at plasmamembrane surface. The normal density present for a certain receptor (A) is down-regulated after strong/continued action of an agonist (B), the receptors are internalized in vesicles or endosomes, where they will be destroyed or reclycled. This is what happens in physiologic situations, like v-adrenoceptor (v-AR) downregulation with aging or after consistent v-AR activation during a marathon run, or in pathologic situations, as in CHF, for the strong sympathetic activation on cardiac v-AR, or during opioid treatment in pain therapy. After the action of an inverse agonist (C), like v-blockers or antihistaminic drugs or prolonged caffeine intake the receptors are expressed with increased density at membrane level. This occurs also in physiological conditions, i.e. exercise training may enhance v-AR in old untrained rats which have spontanous down-regulation (Leosco D, Am J Physiol Heart Circ Physiol 293: H1596H1603, 2007). Common variations of denstiy range from 30-40% less to 30-150% more receptor than basal level, but individual differences are frequent.
Many drugs both agonists or inverse agonists, produce withdrawal syndromes or the parallel phenomenon of rebound effects [16], like beta-blockers, BDZs, opioids, antihistamines, cannabinoids and many others [17] and in most cases receptor adaptations have been demonstrated or suspected. Rebound effects are considered an increase of negative symptoms after drug discontinuation, worse than the pre-treatment conditions. From similar observations about symptoms aggravation after the first benefit of palliative treatments homeopathic theory and method were built [1]. The three following observations are the base for the only theoretical explanation attempted for homeopathy.
Coffee, opium and wine (Organon, par. 65): In these examples coffee produces immediately excessive vivacity but secondarily drowsiness, opium produces heavy sleep but the night after greater insomnia and excessive wine causes heat in the body and the day after chilliness. Coffee contains caffeine, which is an inverse agonist (antagonist) of adenosine receptors (mainly A1R and A2AR). Increasing concentration of adenosine at evening is thought to stimulate A1R in the basal forebrain promoting sleepiness [18]. Inversely caffeine antagonises A1R activity and promotes vigilance and vigor [19]. Chronic caffeine use leads to receptor up-regulation [20, 21] and discontinuation of the intake elicits a withdrawal syndrome with increased drowsiness and decreased alertness, until the next intake [19] (Fig. 1C). Two of opiates most common effects are sedation and drowsiness. Acute or chronic opiates (agonists) readily lead to receptor desensitization or internalization accounting for the secondary symptoms described below. Increased desensitization or decreased reinsertion of receptors to the membrane begin after seconds or minutes of exposure and are considered responsible for tolerance and neuronal hyperexcitation [22, 23]. Correspondingly opiate withdrawal syndrome is characterized by insomnia, diarrhea, anxiety, restlessness. Insomnia, is the first symptom that require medication in withdrawn subjects (60%) [24], and its presence may reach the 100% in this population. It takes 4 weeks or more to fade away. (Fig. 1B). In acute alcohol exposure dominate sedation and vasodilation, but withdrawal symdrome presents hypertension, tremor, shivering and hyperthermia [25]. Acute ethanol inhibits different receptors while chronic exposure upregulate them giving hyperexcitability and tremulousness [26, 27], however other receptor adaptations are more pertinent with thermoregulation. Ethanol acutely inhibits cold-sensitive receptors, TRPM8, probably replicating the action of heat [28]. In literature secondary TRPM8 adaptations to ethanol exposure have not been studied, but if upregulation ensues, as expected after inhibition, it may produce the symptoms of TRPM8 activation, incresed sensitivity to cold, shivering-like muscle activity, skin vasoconstriction, heat-seeking behaviour and increased core temperature, as occured in mice exposed to TRPM8 agonist menthol [29] (Fig 1C). From this analysis seems that, strangely, the first attempt to explain the effects of similar drugs was searched totally indepentently from the issue of dilution, but uniquely from a pharmacologic point of view with high doses. A biological foundation for this ‘effect inversion’ is probably caused by homeostatic inverse receptor adaptations [21]. This analysis confirms that the original interpretation of a body reaction to drugs is biologically founded. Bidirectional receptor adaptations opposite to physiological or pharmacological stimuli are common, quick and widespread in different conditions, like taking coffe or making a strong exercise or after a chronic social stress [30] or, especially, after the intake of drugs. The therapeutic rebound effect (TRE): The second step of Hahnemann’s theory [31] seems a little unclear and artificial but based on his clinical cases and contains the core of his discovery: the rebound effect may be used to treat diseases. The idea was that during diseases body sensitivity to drugs should not be the same than in healthy states, then body reaction to similar drugs after the primary effect can not produce a complete opposite state, anyway it tries to prevail and it is sufficient to restore the normal situation. This effect was considered the healing action of the similar drugs, a secondary reaction of the body contrary to the direction of the similar drug able to rescue health. In the allopathic way, after a first benefit by antagonistic and palliative treatment, secondary actions are in the wrong sense and worsen the disease, making pathologies more chronic. Only using similar drugs the body secondary reactions are in the right sense counteracting the symptoms. Allopathy looks for a direct, fast, short-lasting benefit through contrary medicines but paying the bill of unpleasant secondary reactions that worsen the level of the disease. On the other side homeopathy looks for similar medicines which in the short time may increase the symptoms if the dose is not sufficiently attenuated, but getting the advantage of a long-lasting benefit. Probably this long-term body reaction in the sense of health allows a single dose of a similar drug to last for days or weeks. This hypotethic action of the similar drugs may be correct only if disease alterations consist of different levels of receptor impairments, as it was demonstrated in many chronic diseases like diabetes, heart failure, cancer, neurological diseases (depression, schizophrenia, down symdrome, Alzheimer disease, etc.). Secondarily also conventional non-diluted drugs could be used in a similar paradoxical way to restore receptor alterations and recover health through a reaction of the body. Several examples of these drugs are present in literature for important diseases, but here we have no space to begin this issue. The most important example of a non-diluted, similar drug is the betablocker metoprolol prescribed in heart failure. In this disease a specific beta1-adrenoceptor reduction was shown [32] and metoprolol, a beta1 selective beta-blocker is prescribed. In acute doses it negatively influences heart inotropism, therefore in heart failure initially low doses are given to avoid possible aggravation, but in the long-term a net benefit is achieved in exercise tolerance, symptoms and mortality. Also carvedilol, a non-selective beta-blocker, decreases mortality but was anable to improve symptoms and exercise tolerance nor to increase betareceptors. To restore cardiac beta-receptor down-regulation through a homeostatic rebound effect by antagonists was the idea of the pioneers of this therapy. This idea demonstrated to increase cardiac beta-receptor number [33, 34] and saved thousands of lives. The hypothesis here presented is fifteen years old [35-37] and its weak points have been studied for a long time. Fortunately recent researches have rendered it more probable showing that receptor adaptations (body reactions) are not limited to agonist drugs but also to inverse agonists as it was requested for a complete validation [35]. Another expected confirmation was the interaction of high dilutions with membrane receptors. Standard doses of antagonists have blocked the action of infinitesimal agonists, as Sainte-Laudy and Belon [38] and Mannaioni et al. [39] have succesfully evidenced. Thirdly this model predicts that direction of drug effects should not change for a dilution effect at least in simple systems as in vitro models [38, 39]. This model is also compatible with important homeopathic characteristics, like initial homeopathic aggravation of symptoms during a disease treatment [35], individualization, modalities, totality of symptoms and double effects in 30CH provings as it will be shown in next works.
Bibliography
1. Hahnemann S. Organon of medicine. VI ed. B. Jain Publisher, reprint ed. 1991 (par. 59-66). 2. Dunham C. Homeopathy the science of therapeutics. B. Jain Publisher, reprint ed., 1997. 3. Poitevin B. Le devenir de l’homéopathy. Doin Ed., 1987. 4. see ref. 1, par. 50, 70 and 111. 5. RANG AND DALE’S Pharmacology, 7th ed. Elsevier/Churchill Livingstone, 2012. 6. Almirantis Y. Homeopathy, 102, 114-122, 2013. 7. Bischof M and Del Giudice E. Mol Biol Int, 2013: 987549, 2013. 8. Shin EJ et al. J Pharmacol Sci, 105: 367-371, 2007. 9. Tokay T et al. Neural Plasticity, 2014: 684238, 2014. 10. de Ligt RA et al. Br J Pharmacol, 130:112, 2000. 11. Marchese A et al. Annu Rev Pharmacol Toxicol, 48:601-629, 2008. 12. Cooper JR et al. The Biochemical Basis of Neuropharmacology. 8th ed. Oxford Un. Press, 2003. 13. George CF and Robertson D. Med Toxicol Adverse Drug Exp, 2: 367-382, 1987. 14. Esterlis I et al. Synapse, 63:1089-1099, 2009. 15. Klein RL and Harris RA. Jpan J Pharmacol, 70: 1-15, 1996. 16. Teixeira MZ. Int J High Dilution Res, 11: 69-106, 2012. 17. Hodding GC et al. West J Med, 133: 383-391, 1980. 18. Yang C et al. Front Neurol, vol. 4: article 77, 2013. 19. Sigmon SC, et al. Psychopharmacol, 204: 573-85, 2009. 20. Green RM and Stiles GL. J Clin Invest, 77: 222-227, 1986. 21. Jacobson KA et al. Trends Pharmacol Sci, 17: 108-113, 1996. 22. Roman-Vendrell C et al., J Biol Chem, 287:14782-14791, 2012. 23. Williams JT et al. Pharmacol Rev, 65: 223-254, 2013. 24. Hillhouse M et al. J Addict Dis, 29(1): 23-29, 2010. 25. Bercault N et al. Rev Med Int, 10: 203-205, 1989. 26. Thomas MP et al. J Pharm Exp Ther, 287:87-97, 1998. 27. Walter HJ et al. J Biol Chem, 275: 2571725722, 2000. 28. Weil A et al. Mol Pharmacol, 68: 518-527, 2005. 29. Tajino K et al. Am J Physiol Regul Integr Comp Physiol, 293: R2128-R2135, 2007. 30. Hannibal KE and Bishop MD. Phys Ther, 94:1816-1825, 2014. 31. see ref. 1, end of par. 64, 66 and 112. 32. Bristow MR et al. Circ Res, 59: 297-309, 1986. 33. Heilbrunn SM et al. Circulation, 79: 483-490, 1989. 34. Waagstein et al. Circulation, 80: 551-563, 1989. 35. Signorini A, et al. Homeopathic Links, 13: 227-233, 2000. 36. Signorini A. Int J High Dilution Res. 13: 125-129, 2014. 37. Bellavite P et al. Homeopathy, 104: 139-160, 2015. 38. Saint-Laudy J and Belon P. Homeopathy, 98: 186-197, 2009. 39. Mannaioni PF et al. Med Sci Monit, 16: BR227-232, 2010.
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/281112544
Andrea Signorini
LMHI 2015 RIO DE JANEIRO
![]()
Kevin, nuestro redactor oficial en Farmacia Coliseum, tiene más de 10 años de experiencia en el sector farmacéutico. Con un enfoque claro y accesible, convierte temas complejos en consejos prácticos y útiles, ayudando a nuestra comunidad a mejorar su salud y bienestar.